
Nearly one in three women who struggle to conceive are told the same thing after their HSG test: your tubes are blocked. For most, it is the first time they have even thought about their fallopian tubes. And suddenly, a term they barely knew existed becomes the reason their pregnancy has not happened. If you are searching for blocked fallopian tubes treatment in Wakad, this article gives you a clear picture of what the diagnosis actually means, which treatments work in which situations, and what to expect at each stage of care at 6Venus Fertility Hospital.
What a Blocked Fallopian Tube Actually Does to Fertility
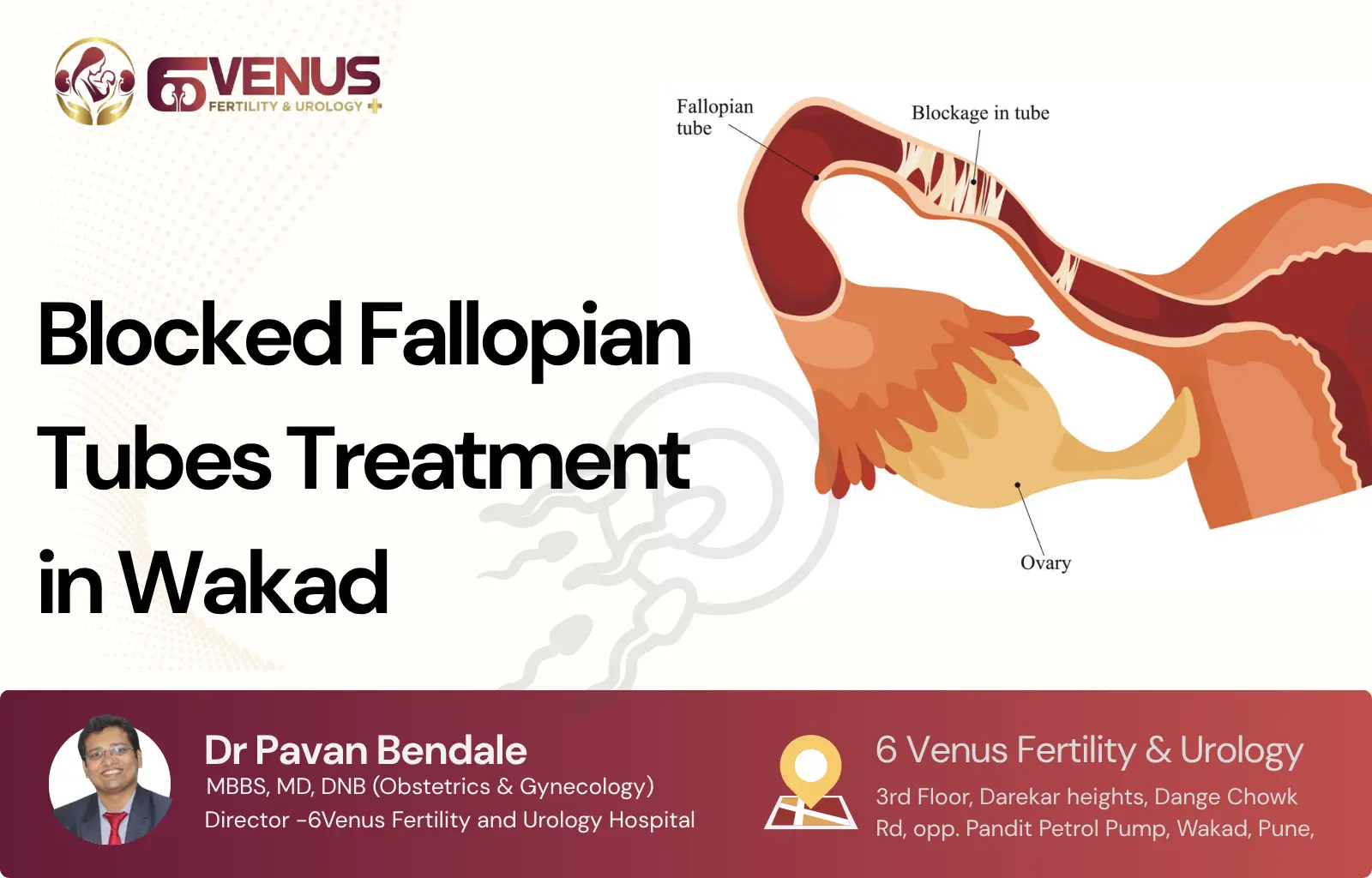
The fallopian tubes are two thin pathways, each roughly 10 centimetres long, that connect your ovaries to the uterus. Every month during ovulation, one of your ovaries releases an egg. The tube on that side catches the egg and moves it toward the uterus. Conception happens inside the tube, not inside the uterus. Sperm travels up from the uterus, enters the tube, and meets the egg there. The fertilised embryo then travels down the tube into the uterus, where it implants and grows into a pregnancy.
When a tube is blocked at any point along this path, that entire sequence breaks down. Sperm cannot reach the egg. The egg cannot travel to the uterus. A fertilised embryo, if one somehow forms, gets trapped inside the tube, which is what causes an ectopic pregnancy. If both tubes are blocked, natural conception becomes impossible without medical help.
What makes fallopian tube blockage particularly difficult is that it usually has no symptoms of its own. Women with partially or fully blocked tubes often have normal periods, no pelvic pain, and no indication anything is wrong until months or years of trying to conceive have passed without success. According to the Mayo Clinic, blocked fallopian tubes account for approximately 25 to 30 percent of all female infertility cases, making tubal occlusion one of the most common structural causes of infertility worldwide.
The Most Common Causes of Fallopian Tube Blockage
Fallopian tube blockage is almost always the result of inflammation, infection, or scarring from a prior event in the reproductive tract. Understanding what caused the blockage is as important as knowing the blockage exists, because the cause directly affects which treatment will work.
Pelvic inflammatory disease (PID) is the leading cause. PID typically develops from sexually transmitted infections, most commonly chlamydia or gonorrhea, that travel up from the cervix and infect the uterus, tubes, and ovaries. The body’s immune response creates inflammation, and after the infection resolves, scar tissue called adhesions forms inside and around the tubes. Even a single episode of PID that went undiagnosed or was treated late can leave permanent blockage.
Endometriosis is another frequent cause. In this condition, tissue similar to the uterine lining grows outside the uterus, including on the surface of the fallopian tubes and nearby structures. This tissue bleeds during menstrual cycles and creates inflammation, scarring, and adhesions that physically block or distort the tubes over time.
Hydrosalpinx refers to a specific type of blockage where the far end of the tube gets sealed shut and fluid accumulates inside, causing the tube to swell. Hydrosalpinx is significant not just because it blocks the tube but because the fluid inside is toxic to embryos, which is why it actively reduces IVF success rates when present.
Other causes include prior pelvic or abdominal surgeries where adhesions formed during healing, ruptured appendix, prior ectopic pregnancy that required surgical intervention, and, rarely, congenital malformations of the tubes present from birth. The location of the blockage, whether it is near the uterus, in the middle section, or at the fimbrial end near the ovary, also affects treatment options significantly.
How Blocked Fallopian Tubes Are Diagnosed in Wakad
There is no symptom that reliably identifies a blocked tube, which is why diagnosis always requires an imaging test or a direct surgical view inside the pelvis.
The hysterosalpingogram (HSG) is typically the first test ordered. During an HSG, a small amount of contrast dye is injected through the cervix into the uterus. If the tubes are open, the dye flows freely through them and spills out near the ovaries, which shows up clearly on X-ray. If a tube is blocked, the dye stops at the point of obstruction. The test is done as an outpatient procedure, usually between day 7 and day 10 of the menstrual cycle, and takes less than 30 minutes. Some women experience cramping during and shortly after the procedure, which is normal and temporary. At 6Venus Fertility Hospital in Wakad, sonography and diagnostic workup are done in-house, making it easier to move quickly from diagnosis to a treatment decision.
The HSG is a screening tool, not a definitive verdict. Spasms in the tube during the procedure can sometimes cause dye to stop temporarily, giving a false positive result for blockage. This is why a second diagnostic step is often recommended before proceeding to surgery.
Laparoscopy is the gold standard for definitive diagnosis. During a laparoscopy, a thin camera is inserted through a small incision near the navel under general anaesthesia. The surgeon can see the tubes directly, assess the degree of damage, check for endometriosis, and evaluate the overall pelvic environment. A dye test called a chromopertubation is typically performed at the same time, where blue dye is pushed through the tubes while the surgeon watches to see where it flows and where it stops. Laparoscopy is both diagnostic and potentially therapeutic because minor blockages can sometimes be cleared during the same procedure.
Blocked Fallopian Tubes Treatment in Wakad: Which Option Is Right for You
Not every blocked tube needs surgery. And not every surgical repair leads to pregnancy. The right treatment depends on where the blockage is located, how severe the damage is, your age, your partner’s sperm quality, and how much time you have available. This is the conversation every patient at 6Venus Fertility Hospital has with Dr. Pavan Bendale before any decision is made.
Tubal Cannulation for Proximal Blockages
Proximal blockages, meaning those located at the point where the tube meets the uterus, are sometimes not true structural blockages at all. Mucus plugs, debris, or temporary spasm can mimic blockage on an HSG. Tubal cannulation addresses this directly. A thin flexible wire is passed through the cervix, into the uterus, and guided into the opening of the tube under fluoroscopic or hysteroscopic guidance. The wire gently opens the pathway and allows dye to pass through, confirming that the tube is actually clear. Tubal cannulation is non-surgical, done without any skin incision, and women typically return home the same day. For proximal blocks caused by mucus or debris rather than true scarring, pregnancy rates after cannulation are reasonably good. If the tube is blocked due to actual scar tissue, however, cannulation is not effective and the approach shifts to laparoscopy or IVF.
Laparoscopic Surgery for Repairable Tubes
Laparoscopic surgery is the most common surgical treatment for blocked fallopian tubes. Through two or three tiny incisions in the abdomen, the surgeon introduces a camera and instruments, and works to repair or open the tube depending on the nature of the blockage.
For tubes blocked by adhesions or scar tissue on their outer surface, the adhesions can be divided and removed, a procedure called adhesiolysis. When the far end of the tube is blocked and hydrosalpinx has developed, the surgeon can create a new opening near the ovary to restore drainage, a procedure called salpingostomy or fimbrioplasty depending on how much of the natural fimbria is preserved.
What matters most in deciding whether surgery is appropriate is the state of the tube underneath the blockage. If the inner lining of the tube has been destroyed by chronic infection or endometriosis, opening the outer blockage does not restore function. A tube that looks open after surgery but has lost its delicate inner cilia will not successfully transport an egg. This is why surgical outcomes vary significantly based on the underlying cause and duration of the blockage. According to research published on PubMed, pregnancy rates after tubal surgery range from 20 to 40 percent in favourable cases but fall considerably when tubes are severely damaged or hydrosalpinx is advanced.
Recovery from laparoscopic surgery is generally faster than from open surgery. If you are considering surgical treatment and want to understand the expenses involved, you can learn more about the costs of various gynecology services including laparoscopic and other gynecological procedures in Punjab through our detailed guide Gynecology Services.
Salpingectomy Before IVF When the Tube Cannot Be Saved
When a tube is severely damaged, particularly when hydrosalpinx is confirmed, removing the tube entirely is often the better decision. This sounds counterintuitive, but the reasoning is medically sound. A tube full of stagnant fluid continuously leaks that fluid into the uterine cavity. The fluid is inflammatory and toxic to embryos. Attempting IVF without removing a hydrosalpinx significantly reduces the chance of implantation. Studies have consistently shown that salpingectomy before IVF improves pregnancy rates in women with hydrosalpinx, which is why removal is now a standard recommendation in such cases. The remaining tube, if healthy, continues to function, and IVF bypasses the need for functional tubes entirely.
IVF: When Bypassing the Tubes Is the Most Efficient Path
IVF does not use the fallopian tubes at all. Eggs are retrieved directly from the ovaries under ultrasound guidance, fertilised with sperm in a lab, and the resulting embryo is placed directly into the uterus. This is why IVF is often the most practical and time-efficient option for women with blocked fallopian tubes, especially those who are older, have bilateral blockage, have partners with sperm issues, or have already attempted surgical repair without success.
At 6Venus Fertility Hospital in Wakad, IVF and ICSI treatment is available with affordable EMI options starting at Rs 9,999 per month. Dr. Pavan Bendale has completed over 2,500 IVF cycles and specialises in complex cases including those involving tubal blockage, endometriosis, and recurrent implantation failure. For women who have spent years trying without success and are now dealing with a blocked tube diagnosis, IVF often offers the most direct and reliable path to pregnancy.
The decision between surgery and IVF is rarely about which is better in general. It is about which is better for a specific patient at a specific point in time. A 28-year-old with a unilateral proximal block and no other fertility factors may benefit from cannulation first. A 36-year-old with bilateral hydrosalpinx and declining ovarian reserve will almost always be better served by salpingectomy followed directly by IVF, without a long waiting period after surgery.
Can You Get Pregnant Naturally With One Blocked Tube?
Yes, and many women do. If one tube is completely clear and the ovary on that side releases eggs regularly, sperm can still travel through the open tube and fertilisation can occur. The challenge is that ovulation alternates unpredictably between ovaries each month, meaning roughly half of your cycles will not result in a viable egg reaching the open tube. Conception can still happen, but it may take longer than in women with two open tubes. If you have one blocked tube and one clear tube, your doctor may recommend a monitored approach where ultrasound confirms which ovary is releasing the egg in a given cycle, focusing timed intercourse or IUI on cycles where the side with the open tube is active.
What to Expect at Your First Consultation for Blocked Fallopian Tubes Treatment at 6Venus, Wakad
When you come in for a consultation with Dr. Pavan Bendale, the first appointment is not about jumping to a treatment. It is about getting the full picture. Both partners are ideally present because male infertility is a contributing factor in nearly 40 percent of cases, and a semen analysis done alongside your fallopian tube investigation ensures no factor is overlooked.
The consultation covers your menstrual history, previous pregnancies or losses, prior infections, surgical history, and any symptoms you have noticed. If an HSG has already been done elsewhere, those results are reviewed carefully. If not, one may be ordered based on clinical findings. From there, a clear treatment plan is discussed, including timelines, realistic expectations for each option, and what the next step should be based on your specific case. Patients from Hinjewadi, Pimpri-Chinchwad, Baner, and Thergaon consistently note that every decision is explained in plain language, and no investigation or procedure is recommended without a clear clinical reason.
If you have been told your tubes are blocked and you are unsure what to do next, a structured evaluation at 6Venus Fertility Hospital in Wakad is the most efficient way to get a clear answer. Blocked fallopian tubes treatment in Wakad, whether surgical or through IVF, is available with the experience and technology to make a real difference.
Frequently Asked Questions About Blocked Fallopian Tubes Treatment
1. Can blocked fallopian tubes open naturally without surgery?
In most cases, no. True structural blockages caused by scarring, adhesions, or hydrosalpinx do not resolve on their own. Some proximal blockages caused by mucus or temporary spasm can clear with tubal cannulation, a non-surgical procedure. Herbal or home remedies have no clinical evidence supporting their effectiveness for structural fallopian tube blockage.
2. How accurate is the HSG test in detecting blocked tubes?
The HSG is a useful screening test but not perfectly accurate. False positives occur when tubal spasm during the procedure mimics a blockage. The test is more reliable for identifying open tubes than for confirming blockages. A laparoscopy with chromopertubation is the definitive diagnostic standard when clinical doubt remains after an HSG.
3. What is the success rate of laparoscopic surgery for blocked fallopian tubes?
Success rates depend heavily on the cause and severity of the blockage. For mild adhesions with intact inner tube structure, pregnancy rates of 20 to 40 percent are reported within 12 to 18 months. For severe hydrosalpinx or extensive tubal damage, surgery has a much lower success rate, and IVF is typically the recommended path forward.
4. Is there any pain during or after the HSG test?
Most women experience cramping during the HSG similar to strong menstrual cramps. The discomfort is usually brief and resolves within hours. Taking a mild painkiller like ibuprofen 30 to 60 minutes before the procedure helps reduce cramping. The test itself takes under 30 minutes and is done as an outpatient procedure.
5. Will removing a blocked fallopian tube affect my chances of getting pregnant through IVF?
No. IVF does not use the fallopian tubes. Removing a tube that contains hydrosalpinx actually improves IVF success rates because the toxic fluid inside reduces embryo implantation rates when left in place. Most fertility specialists recommend salpingectomy before IVF when a hydrosalpinx is confirmed.
6. Can I have IVF with both tubes blocked?
Yes. IVF retrieves eggs directly from the ovaries and bypasses the tubes entirely. Bilateral tube blockage is one of the most common reasons couples proceed directly to IVF, and it does not reduce IVF success rates on its own. Success depends on age, ovarian reserve, and embryo quality, not on whether the tubes are open.
7. How long after laparoscopic tube repair should I wait before trying to conceive?
Most doctors recommend waiting 4 to 6 weeks after the procedure for the pelvis to heal before resuming intercourse. Active attempts to conceive typically begin after 6 to 8 weeks. If pregnancy does not occur within 6 to 12 months of confirmed open tubes post-surgery, IVF is generally the next step, particularly for women over 35.
8. Can endometriosis cause fallopian tube blockage even if it is mild?
Yes. Even mild to moderate endometriosis can produce adhesions around the tubes that interfere with egg pickup by the fimbriae, even when the tube itself is not blocked internally. This is sometimes called functional tubal factor, where the tube appears open on an HSG but does not work normally because of surrounding scarring or distortion.
9. What is hydrosalpinx and why does it matter for IVF?
Hydrosalpinx is a condition where one or both fallopian tubes become blocked at the fimbrial end and fill with fluid. This fluid is inflammatory and leaks into the uterine cavity, where it creates a hostile environment for embryos. Women with untreated hydrosalpinx have significantly lower IVF success rates, which is why removal before IVF is a standard recommendation.
10. How much does blocked fallopian tube treatment cost in Wakad?
Costs vary based on the diagnostic tests required and the treatment approach chosen. An HSG is significantly less expensive than laparoscopic surgery. IVF treatment costs depend on the number of cycles and medications involved. At 6Venus Fertility Hospital in Wakad, IVF packages are available with EMI options starting at Rs 9,999 per month, and all treatment costs are discussed transparently before any procedure begins. Contact the clinic directly for a personalised cost estimate based on your diagnostic reports.


