
Kidney stones are one of the most painful and prevalent urological conditions affecting adults worldwide. If you or a loved one has been diagnosed with a renal calculus (kidney stone), the immediate concern is often how to get rid of it safely and quickly. While small stones often pass on their own with hydration, larger or stubborn stones require medical intervention.
For decades, the standard of care was open surgery or early forms of keyhole surgery. However, the last few years have seen a technological revolution in urology with the advent of high-power lasers. Today, patients are often faced with a choice: Traditional Stone Surgery (PCNL) or Modern Laser Stone Surgery (RIRS/URSL).
This article breaks down the differences, benefits, risks, and recovery processes of both methods to help you understand which might be the right choice for your specific condition.
1. Understanding the Contenders
Before diving into the comparison, it is essential to understand what these procedures actually entail. The term “surgery” can be frightening, but modern urological procedures are far less invasive than they were twenty years ago.
What is Traditional Stone Surgery (PCNL)?
When urologists speak of “traditional” surgery for kidney stones today, they rarely mean open surgery (where a large cut is made on the abdomen). Open surgery is now obsolete for 99% of cases. instead, “Traditional” usually refers to Percutaneous Nephrolithotomy (PCNL).
The Procedure: PCNL is a “keyhole” surgery. The surgeon makes a small incision (about 1 cm) in the patient’s back (flank area). Through this incision, a track is created directly into the kidney. A hollow tube (sheath) is inserted, and a nephroscope (camera) is passed through it to visualize the stone. The stone is then broken using pneumatic or ultrasonic energy (similar to a mini-jackhammer) and the fragments are physically pulled out with forceps.
Best Suited For:
- Very large stones (usually > 20mm or 2cm).
- Staghorn calculi (stones that branch out and fill the kidney).
- Hard stones that lasers might take too long to dust.
What is Laser Stone Surgery (RIRS / URSL)?
Laser surgery represents the minimally invasive evolution of stone treatment. The most common forms are RIRS (Retrograde Intrarenal Surgery) and URSL (Ureteroscopic Lithotripsy).
The Procedure: This is a “no-cut” procedure. The surgeon inserts a thin, flexible tube called a ureteroscope through the natural urinary passage: entering the urethra, passing through the bladder, and moving up the ureter directly into the kidney. Once the scope locates the stone, a high-power laser fiber (Holmium or Thulium laser) is passed through the scope. The laser energy vaporizes the stone into fine dust (dusting) or breaks it into tiny fragments that pass out naturally with urine.
Best Suited For:
- Small to medium-sized stones (< 20mm).
- Stones in difficult locations (like the lower pole of the kidney).
- Patients on blood thinners or those who cannot tolerate cuts.
- Patients demanding the quickest cosmetic and functional recovery.
2. Head-to-Head Comparison: Laser vs. Traditional
To decide which is “best,” we must evaluate them across several critical categories: invasiveness, pain, recovery, and success rate.
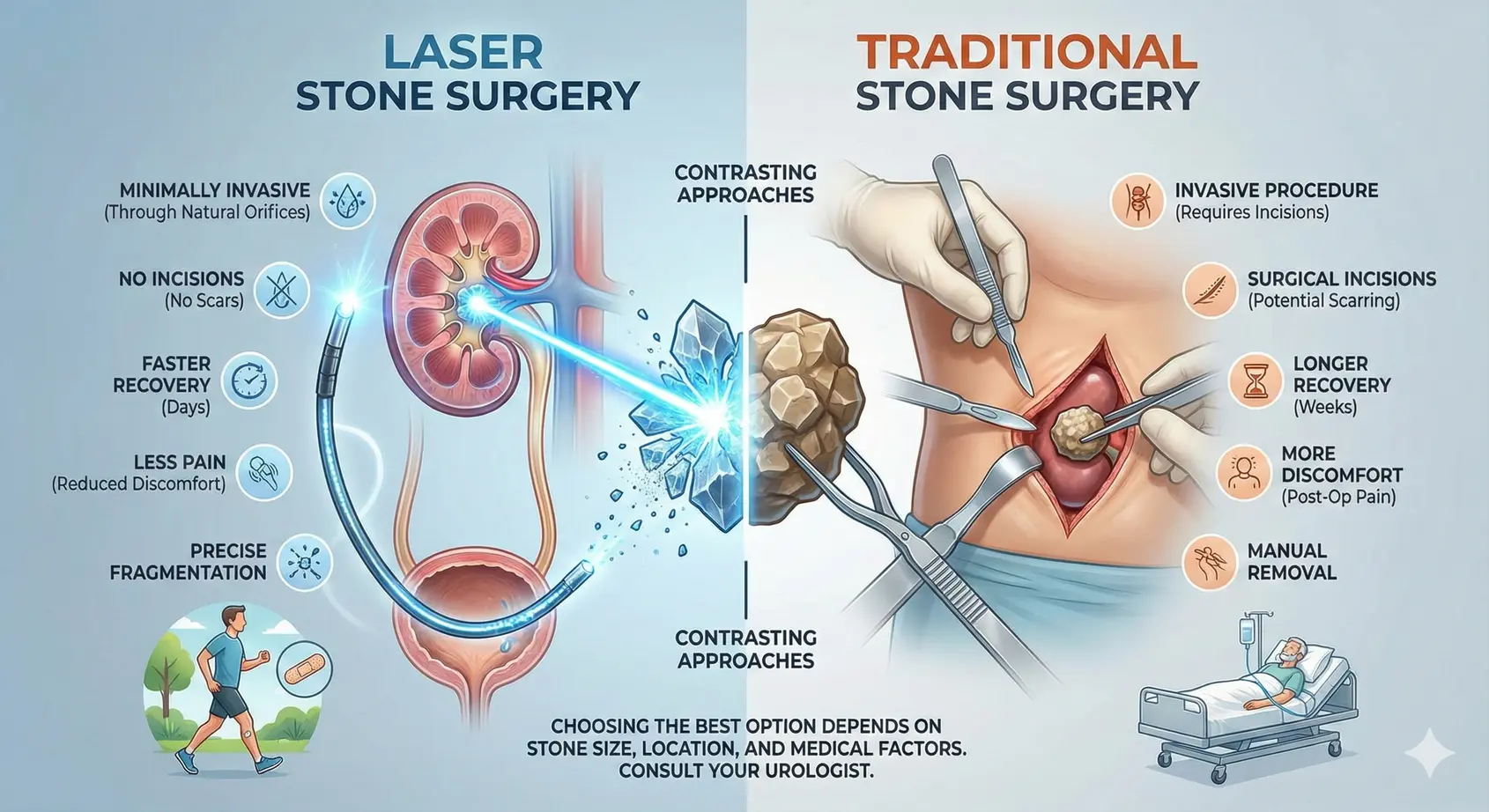
A. Invasiveness and Scarring
- Traditional (PCNL): This is an invasive procedure. It requires a puncture wound in the kidney and a cut on the skin. While the scar is small (1 cm), there is still trauma to the kidney tissue and the muscles of the back.
- Laser (RIRS): This is completely non-invasive regarding skin cuts. It utilizes the body’s natural orifices. There are no external scars, no stitches, and no bandages required post-surgery.
- Winner: Laser (for cosmetic results and zero incisions).
B. Pain and Discomfort
- Traditional (PCNL): Because a tube is placed through the back muscles into the kidney, there is moderate postoperative pain. Patients typically require injectable painkillers for the first day and oral painkillers for a few days after. A drainage tube (nephrostomy tube) is often left hanging from the back for 1-2 days, which can be uncomfortable.
- Laser (RIRS): Pain is significantly less. Most patients describe it as a mild heaviness or discomfort rather than acute pain. There is no external tube. However, a temporary internal stent (DJ stent) is placed to keep the ureter open, which can cause mild irritation or urinary urgency, but this is generally well-tolerated.
- Winner: Laser (significantly less pain).
C. Hospital Stay and Recovery
- Traditional (PCNL):
- Hospitalization: Usually 2 to 3 days. You are monitored for bleeding and urine output.
- Recovery: Complete recovery takes about 10–14 days. Patients are advised to avoid heavy lifting for at least 2 weeks to allow the kidney puncture to heal.
- Laser (RIRS):
- Hospitalization: Often performed as a “Day Care” procedure (discharged the same evening) or a 24-hour stay.
- Recovery: Most patients return to their desk jobs or daily routine within 2–3 days. Since there is no wound to heal, physical movement is not restricted as strictly.
- Winner: Laser (faster return to normal life).
D. Stone Clearance Rate (Success)
This is where the debate gets interesting.
- Traditional (PCNL): For large stones (>2cm), PCNL is the king. It allows the surgeon to physically remove large chunks of stone. The clearance rate for massive stones is nearly 95-98% in a single sitting.
- Laser (RIRS): For stones <1.5cm, the success rate is equally high (95%+). However, for very large stones (>2.5cm), laser surgery might require two sessions because dusting a massive stone takes hours and can stress the kidney.
- Winner: Tie (PCNL wins for big stones; Laser wins for small/medium stones).
E. Complications and Safety
- Traditional (PCNL): The main risk is bleeding. Since the kidney is very vascular, puncturing it can sometimes hit a vessel. In rare cases (<1%), a blood transfusion is needed. It is generally not safe for patients on blood thinners.
- Laser (RIRS): The risk of bleeding is negligible. The main risks are minor infection (UTI) or mild injury to the ureter (scratching). It is considered the safer option for high-risk patients (elderly, diabetic, or cardiac patients).
3. Which Procedure is Right for You?
The “best” surgery is not a one-size-fits-all answer. It depends entirely on the clinical presentation of your stone. Your urologist will look at your CT scan (NCCT KUB) and recommend a path based on these factors:
Choose Laser Surgery (RIRS) If:
- Your stone is smaller than 20mm. This is the “Gold Standard” zone for laser.
- You want zero cuts. If you are worried about scars or surgery in general, this is the most patient-friendly option.
- You have a strict work schedule. If you need to be back at work by Monday after a Friday surgery, laser is the way to go.
- You are on blood thinners. If you take medication like Aspirin or Clopidogrel for heart issues, stopping them might be risky. Laser can often be done without stopping these drugs (or with a shorter pause) compared to PCNL.
- The stone is in a tricky spot. Flexible scopes can bend 270 degrees to reach “lower pole” stones that rigid instruments cannot reach.
Choose Traditional Surgery (PCNL) If:
- Your stone is massive (>25mm). Laser might turn a large stone into too much dust, which can block the kidney (Steinstrasse). PCNL clears the bulk efficiently.
- You have a “Staghorn” Calculus. These are complex, branching stones that fill the kidney. PCNL is required to clear the bulk of the infection and stone burden.
- Cost is a major factor. In some regions, standard PCNL can be slightly more economical than RIRS because RIRS uses expensive disposable equipment (flexible scopes and laser fibers). However, the cost gap is closing rapidly.
4. The “Mini-PCNL” – A Middle Ground?
It is worth noting that medical technology is constantly evolving. There is now a hybrid technique called Mini-PCNL. In this procedure, urologists use a “miniaturized” version of the PCNL equipment. The incision is smaller (like a needle puncture), and a laser is used through the back incision. This offers the best of both worlds: the ability to tackle larger stones (like standard PCNL) with less bleeding and faster recovery (closer to RIRS). If you have a borderline stone (e.g., 2.2 cm), ask your urologist if Mini-PCNL is an option.
5. What to Expect After Surgery?
Regardless of the method chosen, postoperative care is vital for preventing recurrence.
The Stent Factor: In almost all Laser surgeries and many PCNL surgeries, a DJ Stent (Double-J Stent) is placed inside the ureter. This is a thin, soft plastic tube that ensures urine drains from the kidney to the bladder while the swelling subsides.
- Sensation: You cannot see the stent, but you might feel it. It can cause a frequent urge to pass urine or a slight prickly sensation in the bladder at the end of urination.
- Removal: The stent is temporary and is usually removed 10–14 days after surgery via a minor procedure that takes 2 minutes.
Dietary Changes: Once the stone is removed, it should be sent for analysis. Knowing the composition (Calcium Oxalate, Uric Acid, etc.) helps in planning your diet.
- Hydration: The universal rule is to drink 3–4 liters of water daily.
- Salt: Reduce sodium intake, as salt creates calcium stones.
- Protein: Limit animal protein (red meat) if you have uric acid stones.
Conclusion
The debate between Laser and Traditional Stone Surgery is not about which is “better” in the abstract, but which is “better for the specific stone.”
- Laser (RIRS) is the champion of comfort, safety, and speed for small to medium stones. It is the modern choice for the busy individual who values a non-invasive approach.
- Traditional (PCNL) remains the heavy lifter, essential for clearing large, complex stone burdens that laser cannot handle efficiently.
At our facility, we specialize in advanced urological care, offering state-of-the-art Holmium and Thulium laser technologies alongside standard PCNL. We believe in a patient-centric approach—choosing the method that guarantees the highest stone-free rate with the lowest risk to your health.
If you are suffering from flank pain, blood in urine, or have been diagnosed with a kidney stone, do not wait for the damage to worsen. Early intervention often allows for the simpler, laser-based treatment options before the stone grows too large.
Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified urologist for diagnosis and treatment options tailored to your specific medical history.

