
Wakad is one of Pune’s fastest-growing residential corridors. Most of its residents work shifts in Hinjewadi or log hours remotely for IT companies in Pimpri-Chinchwad. They eat late. They sit most of the day. Their stress levels are high and their sleep schedules are irregular. None of this is news to them. What many do not expect is a doctor quietly linking those exact habits to why a pregnancy has not happened – or why, if IVF has already been tried, it did not work as expected.
The IVF success rate in Wakad is not a single number. It cannot be. Two couples sitting in the same waiting room at 6Venus Fertility and Urology Hospital may have wildly different outcomes from the same procedure- because their age, diagnosis, sperm quality, ovarian reserve, and lifestyle history are all completely different. A 29-year-old woman with PCOS and a normal AMH has a very different success picture than a 38-year-old with low ovarian reserve and a partner with poor sperm morphology. The brochure number does not apply to both.
Dr. Pavan Bendale, who has completed over 2,500 IVF cycles at 6Venus and previously at leading fertility centres in Pune, makes this point to every couple who walks in for a first consultation. The question is not “what is your success rate?” The more useful question is “what is my success rate, given my specific reports?”
Why Wakad Couples Are Increasingly Showing Up at Fertility Clinics Earlier
Something has shifted in the past five to six years in the western Pune corridor. Couples in their late twenties and early thirties from Wakad, Hinjewadi, and Pimple Saudagar are now seeking fertility evaluations earlier than previous generations did – often not because they have tried for a long time without success, but because they have seen it happen to friends or colleagues.
A software engineer who sits at a desk for 10 hours a day, eats dinner past 10 PM, and handles client escalations on a rolling basis is not living in a fertility-friendly environment. Neither is his partner, who may be managing her own career, hormonal imbalance from irregular sleep cycles, and the weight of family pressure about timing. PCOS rates among urban Indian women are estimated at 20-30% in the reproductive age group. Sperm quality decline in young men is now well-documented in research tied to sedentary behaviour, heat exposure from laptops, and chronic stress.
At 6Venus, Dr. Bendale has noted that a significant portion of couples presenting from Wakad and Hinjewadi have at least one identifiable lifestyle-linked fertility factor alongside any structural or hormonal diagnosis. This does not mean lifestyle change alone resolves infertility. But it does mean that understanding it as part of the clinical picture affects both diagnosis and protocol design – and therefore, success rates.
IVF Success Rates in Wakad by Age – What the Numbers Actually Mean
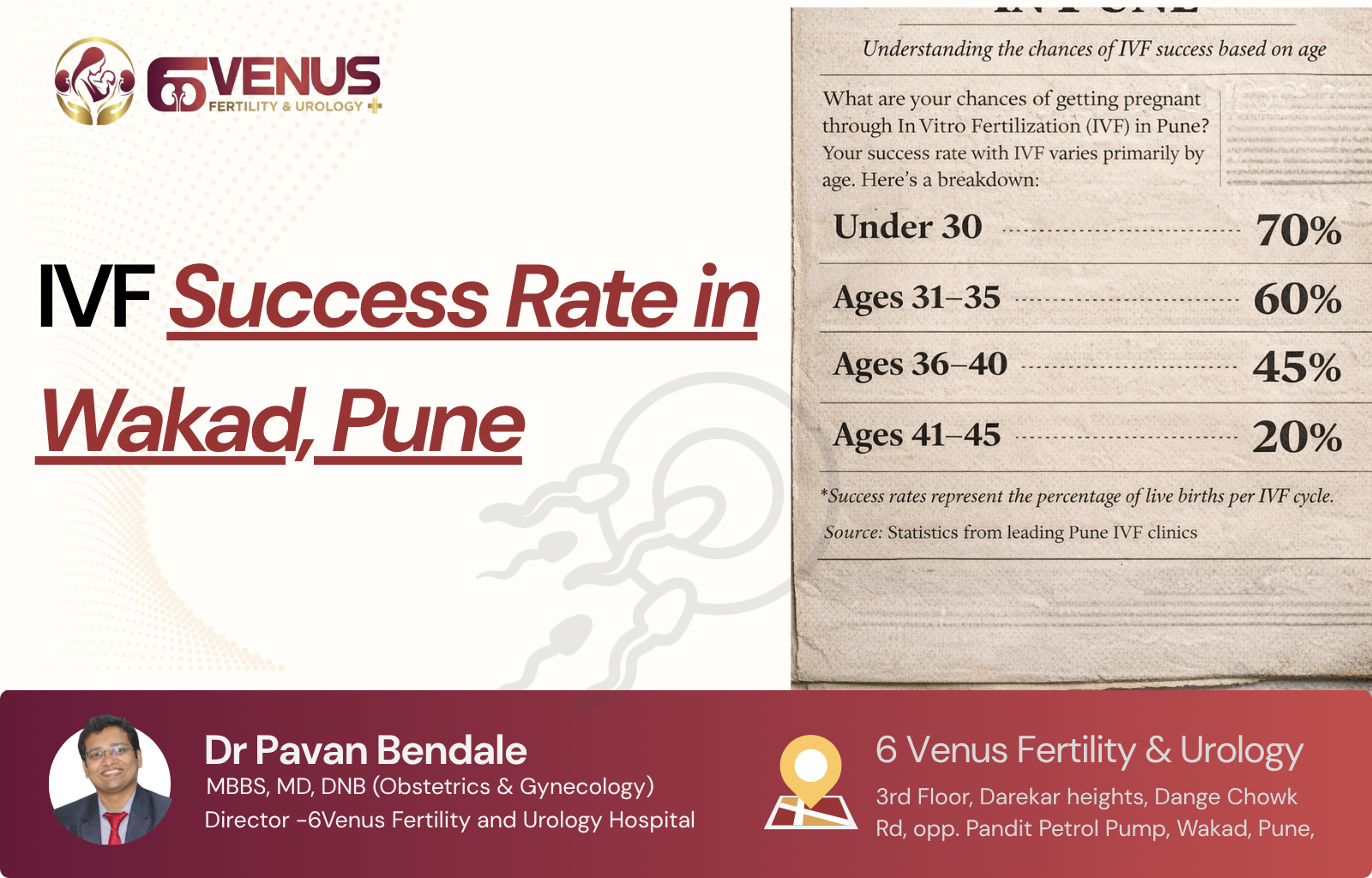
Age is the strongest single predictor of IVF outcome. This is not a marketing caveat – it is the biological reality of how egg quality and ovarian reserve decline over time. Here is what per-cycle live birth rates look like across age groups at specialist fertility centres in Pune, including 6Venus:
| Age Group | Approx. IVF Success Rate Per Cycle | Key Clinical Notes |
|---|---|---|
| Under 30 | 50-60% | Best egg quality, strong ovarian reserve, highest implantation rates |
| 30-34 | 45-52% | Still excellent results; PCOS-related cases respond very well |
| 35-37 | 35-45% | Egg quality begins to decline; PGT increasingly beneficial |
| 38-40 | 25-35% | Stimulation response less predictable; blastocyst transfer recommended |
| 40-42 | 15-20% | Higher chromosomal error rate in embryos; PGT significantly helps |
| Above 42 | Below 10% (own eggs) | Donor egg IVF can restore rates to 60-70%; discussed case by case |
These figures represent per-cycle live birth rates at specialist clinics – not clinical pregnancy rates, which count a heartbeat on ultrasound and are a higher number. The distinction matters. A live birth rate is the number that actually measures what the couple came in for. As Mayo Clinic confirms, women under 35 consistently see the strongest IVF outcomes, and success declines with age in ways that no stimulation protocol fully compensates for.
For couples in Wakad who have been delaying IVF – waiting for the “right time,” a salary hike, or an apartment purchase to settle – this age trajectory is the most important clinical fact to sit with. The right time for IVF, medically speaking, is almost always earlier than it feels emotionally or financially.
The Wakad IT Lifestyle and Its Specific Impact on IVF Success Rate
This section exists because no competitor article on IVF success rates covers it. Generic content talks about age and embryo quality. It does not talk about the specific fertility risks that come with the lifestyle a large chunk of Wakad’s population actually lives.
Here is what the clinical evidence says about the habits common to IT professionals in Wakad, Hinjewadi, and the broader PCMC corridor:
- Prolonged sitting: Men who sit for more than 6 hours a day show measurably higher scrotal temperatures, which damages sperm DNA. Laptops on laps worsen this further. Sperm DNA fragmentation – a parameter many clinics do not test by default – is elevated in this population and directly reduces IVF success rates even when basic semen analysis looks normal.
- Irregular sleep: Night shifts and inconsistent sleep schedules disrupt melatonin and cortisol cycles. In women, this suppresses LH surge quality and can impair ovulation. In men, testosterone is produced primarily during deep sleep – chronic sleep disruption lowers testosterone and degrades sperm production over time.
- Chronic work stress: Sustained cortisol elevation disrupts the hypothalamic-pituitary-gonadal axis – the hormonal cascade that governs both ovulation and sperm production. This is not psychological. It is an endocrine mechanism.
- Late-night eating and weight gain: Visceral fat increases aromatisation of testosterone to estrogen in men, reducing sperm quality. In women, obesity is associated with insulin resistance, which worsens PCOS and suppresses ovarian response to stimulation.
- Low physical activity: Regular exercise improves both egg quality and sperm parameters. Most desk-bound IT workers in Wakad get under 5,000 steps a day.
At 6Venus, Dr. Bendale addresses these factors directly as part of pre-cycle planning. The 6Venus article on male infertility in Pune IT professionals goes into specific detail on how sitting hours and night shifts affect sperm quality – a page worth reading for any male partner before a consultation.
What Actually Determines IVF Success at 6Venus in Wakad
Age is the starting point, not the full picture. These are the clinical factors Dr. Bendale evaluates that directly shape a couple’s realistic IVF success rate in Wakad:
1. Ovarian Reserve (AMH and AFC)
Anti-Mullerian Hormone (AMH) is the best single blood test indicator of how many eggs remain in the ovaries. Antral follicle count (AFC) – done via transvaginal ultrasound – confirms it. Low AMH does not mean IVF is impossible. It means the stimulation protocol needs to be designed more carefully to retrieve maximum usable eggs, and the expectations around egg yield need to be set realistically. Women with very low AMH may need higher stimulation doses, longer protocols, or banking across multiple cycles before attempting transfer.
2. Embryo Quality – Day 3 vs Blastocyst Transfer
Not all embryos are equal. An embryo that looks good on Day 3 of culture may arrest and never develop further. A blastocyst – an embryo that survives to Day 5 – has already passed one major developmental selection filter. Blastocyst transfer consistently shows higher implantation rates than Day 3 transfer across IVF literature. At 6Venus, extended culture to blastocyst stage is recommended whenever the number of embryos supports it. The 6Venus deep-dive on embryo quality and what it means for IVF outcomes explains how the grading system works and why it matters for your specific cycle.
3. Sperm DNA Fragmentation
This is the most commonly missed diagnostic step in Wakad and across India. A standard semen analysis checks count, motility, and morphology. It does not check sperm DNA fragmentation – the degree of damage to the genetic material inside the sperm. High DNA fragmentation leads to poor embryo development and increased early pregnancy loss even when fertilisation appears successful. It is particularly relevant in IT professionals with sedentary lifestyles, high heat exposure, and poor sleep. When fragmentation is high, ICSI with specially selected sperm or antioxidant supplementation before the cycle can meaningfully improve outcomes.
4. Uterine Health Before Transfer
An embryo can only implant in a receptive, structurally normal uterus. Polyps, fibroids, adhesions, a thin endometrium, or a uterine septum can all prevent or reduce implantation without showing obvious symptoms beforehand. At 6Venus, hysteroscopy is recommended before transfer when there is any clinical reason to suspect uterine pathology – particularly in couples with unexplained failure or women with a history of heavy periods, irregular bleeding, or previous uterine surgery.
5. Protocol Design Specific to Your Ovarian Response
One of the factors that separates a specialist fertility centre from a general clinic is the ability to read mid-cycle response and adjust. If a woman is under-responding to stimulation on Day 6, the dose needs to go up. If she is hyper-responding and OHSS risk is rising, the protocol may need to shift to a freeze-all cycle to protect her safety and give the uterus a cleaner environment for transfer. This real-time clinical decision-making is not possible in a clinic doing 2-3 IVF cycles per month. Dr. Bendale’s experience across 2,500+ cycles at 6Venus gives him a large reference base for these decisions.
6. Pre-implantation Genetic Testing (PGT)
For women over 37, or couples with recurrent pregnancy loss or failed cycles, PGT substantially improves the live birth rate per transfer by ensuring only chromosomally normal embryos are transferred. The per-cycle success rate may look similar with or without PGT. But the per-transfer success rate – and the reduction in miscarriage risk – shifts significantly in favour of PGT. See the 6Venus perspective on IVF success factors from a Pune specialist for how these decisions are made at the clinical level.
What a Real 6Venus Patient Said About Her IVF Experience in Wakad
One patient whose story appears on the 6Venus website described her experience this way:
“Coming to the IVF center in Wakad wasn’t an easy decision. We delayed it for months. I kept thinking maybe next cycle would be the one. When we finally came in, the doctor explained things in a way that made sense. He imposed no urgency, no pressure. Just facts – what were true in reports. IVF wasn’t quick or emotionally easy. Some days I felt hopeful, other days I felt numb. The waiting was the hardest part. But having a plan helped. Knowing what we were doing and why helped even more. It didn’t happen instantly for us. But it did happen.”
This account captures something that aggregate success rate numbers do not: IVF success is not only biological. The clarity of information, the honesty of the doctor, and the feeling of being treated as a person rather than a case file all affect how couples navigate the emotional reality of treatment – which in turn affects compliance, stress levels, and ultimately outcomes.
6Venus reports a 98% patient satisfaction rate across its fertility and urology practice. That number does not mean every patient got pregnant. It means nearly every patient felt treated with transparency, respect, and clinical seriousness – regardless of outcome.
IVF Success Rate After a Failed Cycle: What Wakad Couples Need to Know
A single failed IVF cycle does not mean IVF will not work for you. It means the first attempt, with whatever protocol and embryos were available, did not result in a pregnancy. Those are two very different statements.
Cumulative success rates – the probability of a live birth after two or three complete IVF cycles, including frozen embryo transfers from the same retrieval – are significantly higher than per-cycle rates. Published data consistently shows cumulative rates of 65-70% after three full cycles in women under 38. After 40, those cumulative numbers are lower, but the trajectory still improves with subsequent attempts.
When a cycle fails at 6Venus, Dr. Bendale conducts a structured review:
- How many eggs were retrieved and what was the maturity rate?
- How many fertilised and what was the Day 3 embryo count?
- How many reached blastocyst stage and what were the grades?
- Was the endometrial lining adequate on transfer day?
- Were there any unusual lab findings during culture?
- Is sperm DNA fragmentation testing indicated now if not done before?
- Is hysteroscopy warranted before the next transfer?
- Does the failure pattern suggest PGT should be added to the next cycle?
The answer to these questions shapes the next protocol. Simply repeating the same cycle with the same approach after a failure is not a clinical strategy – it is a lottery. See more on what happens when embryos repeatedly fail to implant in the 6Venus article on embryo implantation failure.
Lifestyle Changes That Actually Move the IVF Success Needle in Wakad
For the couple in Wakad who has been told to “reduce stress and eat healthy” without any specifics, here is what the evidence actually supports in the 60-90 days before an IVF cycle:
- For the male partner: Stop using a laptop directly on the lap. Take short walks every 90 minutes of sitting. Get 7-8 hours of sleep consistently. Add CoQ10 (200-400mg/day) and Vitamin C, D, E supplements 3 months before the cycle – sperm takes 74 days to complete one production cycle, so changes made today affect the sperm used in your IVF retrieval 10 weeks from now.
- For the female partner: Maintain a BMI between 19-25. Add folate (or methylfolate if MTHFR mutation is known) 3 months before stimulation. Reduce refined carbohydrates if PCOS is present – insulin sensitivity improvement directly improves ovarian response. See the detailed 6Venus fertility diet plan for Pune patients for specific food guidance.
- Both partners: Alcohol significantly reduces embryo quality. Stop entirely for at least 3 months before a cycle. Smoking – including passive exposure – damages both egg and sperm quality. Sleep before midnight; the growth hormone and testosterone release window is between 10 PM and 2 AM.
These are not platitudes. Each of these has a measurable biological mechanism. None of them replace medical treatment. But for Wakad couples whose lifestyle includes several of these risk factors, addressing them before the cycle meaningfully improves the baseline that treatment is working with.
Choosing a Fertility Clinic in Wakad Based on Success Rate: What to Ask
When a clinic quotes you a success rate, ask these five questions before trusting the number:
- Is this a clinical pregnancy rate or a live birth rate? A heartbeat on ultrasound is not the same as a baby born at home. Insist on live birth rates.
- Is this rate for all age groups combined, or age-specific? A clinic that treats mostly younger patients will show higher aggregate rates than one that handles complex and older-patient cases. Age stratification is the only fair comparison.
- Does this include frozen embryo transfers, or fresh cycles only? FET cycles are often more successful than fresh transfers in specific patient groups. A combined figure tells a different story than fresh-only data.
- What percentage of your patients have previously failed IVF cycles elsewhere? A clinic that takes on referred difficult cases will show lower success rates than one that refuses complex presentations. Lower rates in this context actually reflect clinical courage, not poor quality.
- What is your cancellation rate? Poor response cycles that are cancelled before retrieval are not always included in published success denominators. High cancellation rates can artificially inflate apparent success percentages.
At 6Venus’s IVF centre in Wakad, Dr. Bendale discusses these questions openly in the initial consultation. He does not hand over a printed success rate brochure and move on. He reviews your specific reports and gives you a realistic assessment of what your individual cycle is likely to look like – which is the only information that actually helps you make a decision.
The One Thing About IVF Success That Most Articles Do Not Say
IVF success rate is not the number on a clinic’s website. It is the probability that applies to your specific age, diagnosis, embryo count, uterine health, and treatment protocol – at the hands of a doctor who has seen enough cycles to read the clinical signals correctly.
Wakad has a concentrated population of educated, working couples who research extensively before making medical decisions. They read everything. They compare clinics. They ask good questions. That is a strength. But the one thing that no amount of research replaces is a consultation where a doctor reads your actual reports and tells you honestly what your picture looks like.
If you are in Wakad, Hinjewadi, Pimple Saudagar, Marunji, or anywhere in the PCMC corridor, and the question of IVF success rate is on your mind, the most direct path to a real answer is a consultation with Dr. Pavan Bendale at 6Venus Fertility and Urology Hospital on Dange Chowk Road, Wakad. He will not give you a number off a pamphlet. He will give you an assessment that actually applies to you.
10 Questions Wakad Couples Ask About IVF Success Rate – Answered
1. What is the IVF success rate in Wakad for a first cycle?
For women under 35 with no severe pathology, IVF success rates at specialist clinics in Wakad run approximately 45-55% per cycle. For women 35-38, expect 30-45%. Above 40, rates with own eggs typically fall below 20%. These are population averages. Your individual rate depends on AMH, antral follicle count, sperm quality, uterine health, and the protocol your doctor designs. At 6Venus, Dr. Bendale gives you an estimate based on your actual reports, not a population average.
2. Does the IVF success rate improve after a failed first cycle?
Cumulative success rates do increase with additional cycles. Published data shows cumulative live birth rates of 65-70% after three complete cycles in women under 38. A failed first cycle also gives the doctor valuable clinical information – about how your ovaries responded, how embryos developed, and what can be adjusted in the next protocol. At 6Venus, every failed cycle is formally reviewed before a second attempt begins.
3. Is the IVF success rate different for IT professionals in Wakad?
Not as a category – IVF success is not determined by profession. But the lifestyle factors common in IT work – prolonged sitting, sleep disruption, chronic stress, late eating – do measurably affect egg quality, sperm DNA integrity, and hormonal balance. These can lower the starting baseline before treatment begins. Addressing them in the 60-90 days before a cycle is one of the most underutilised ways to improve outcomes.
4. Does PCOS affect IVF success rate in Wakad couples?
PCOS affects the stimulation phase more than the success rate itself. Women with PCOS often produce many follicles in response to stimulation, but OHSS risk is higher. With careful protocol management, blastocyst culture, and a freeze-all cycle if needed, PCOS patients can achieve excellent outcomes. In fact, because PCOS patients usually have good ovarian reserve, egg yield is often high – which means more embryos to select from. The key is choosing a clinic with experience managing PCOS stimulation safely. See the 6Venus overview of PCOS causes and lifestyle factors in Pune.
5. How does sperm quality affect the IVF success rate?
Significantly. Poor sperm morphology, low motility, or high DNA fragmentation reduces fertilisation rates and embryo quality even when the female partner’s parameters are normal. ICSI helps when morphology or count is poor. But high DNA fragmentation – which standard semen analysis does not measure – can still limit outcomes even with ICSI. At 6Venus, male fertility evaluation includes DNA fragmentation testing where indicated, and the urology team manages any underlying male factor directly.
6. What is the IVF success rate with frozen embryo transfer (FET) vs fresh?
For many patient profiles, frozen embryo transfer (FET) success rates are comparable or slightly higher than fresh transfers. This is because the uterine environment after a stimulation cycle is sometimes suboptimal – elevated progesterone or estrogen from the stimulation phase can reduce endometrial receptivity. A FET cycle allows the uterus to recover and be prepared fresh for transfer. At 6Venus, the decision between fresh and frozen transfer is made based on your specific endometrial response and hormone levels at the time of retrieval.
7. Does PGT improve IVF success rate in Wakad?
Per transfer, yes – substantially for specific groups. PGT filters out chromosomally abnormal embryos before transfer, which are the most common cause of implantation failure and early miscarriage. For women over 37, those with 2+ prior failed cycles, or couples with a history of miscarriage, PGT improves live birth rate per transfer and reduces time-to-pregnancy by avoiding transfers of embryos that would not implant anyway. The cost is higher per cycle, but the medical and emotional cost of repeated failed transfers often outweighs it.
8. Can lifestyle changes before IVF improve the success rate?
Yes, in measurable ways. Stopping alcohol and smoking 3 months before the cycle, adding antioxidant supplements, normalising BMI, improving sleep, and addressing sperm heat exposure all have published evidence of improving egg quality, sperm DNA integrity, and stimulation response. These changes work through the actual biological production cycle of eggs (around 90 days) and sperm (74 days). The fertility diet plan at 6Venus for Pune patients covers specific recommendations in detail.
9. What is the IVF success rate with donor eggs for older women in Wakad?
Donor egg IVF can restore success rates to 60-70% per cycle even for women over 42, because the limiting factor – egg quality – is bypassed by using eggs from a younger, screened donor. The recipient’s uterine health and endometrial receptivity remain important, but when those are good, outcomes with donor eggs are substantially better than with a woman’s own eggs after 40. At 6Venus, Dr. Bendale discusses donor egg IVF honestly and specifically when a woman’s ovarian reserve or egg quality makes it the most realistic path to a successful pregnancy.
10. How do I know which IVF clinic in Wakad will give me the best success rate?
Ask for age-stratified live birth rates, not aggregate clinical pregnancy rates. Ask whether they handle complex cases or primarily straightforward ones. Ask about cancellation rates. Ask how a failed cycle is reviewed and what changes are made. Ask whether both partners are evaluated from day one. The clinic that answers these questions directly, without evasion, is likely to be more trustworthy than one that leads with a single headline number. At 6Venus, all of these questions are addressed in the first consultation with Dr. Bendale.


